“It takes force, mighty force, to restrain an instinctual animal in the moment of performing a bodily function, especially birth. Have we successfully used intellectual fear to overpower the instinctual fear of a birthing human, so she will now submit to actions that otherwise would make her bite and kick and run for the hills?”
–Sister Morningstar (in Midwifery Today)
 When I end my introduction to human services class and then again when I begin my social policy class, I ask my students to consider the above: What would happen if everyone cared? What would happen if our first reaction was compassion? What would happen if we focused on what matters? What would happen if we assumed everyone had inherent worth and value and deserves humane care and compassion?
When I end my introduction to human services class and then again when I begin my social policy class, I ask my students to consider the above: What would happen if everyone cared? What would happen if our first reaction was compassion? What would happen if we focused on what matters? What would happen if we assumed everyone had inherent worth and value and deserves humane care and compassion?
I have said for a long time that women’s rights in birth represent a human rights issue, so I was very interested to receive word of a Human  Rights in Childbirth campaign:
Rights in Childbirth campaign:
Women do not lose their basic human rights once they become pregnant. And yet, across the globe, women’s human rights are compromised and violated around childbirth. Examinations, interventions and procedures that pose risks to both mothers and their babies are routinely performed without informed consent, or through coerced compliance via threats or fear. When women come out of childbirth with post-partum PTSD from disrespect, abuse, or obstetric violence, the goal of a “healthy mother and healthy baby” has not been met.
via Home | Human Rights in Childbirth.
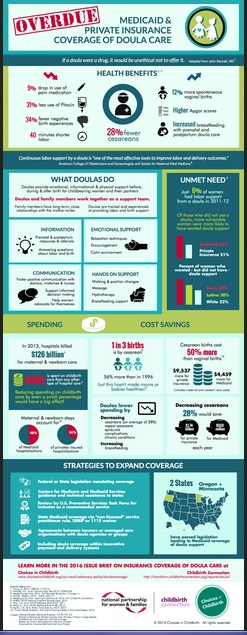
Childbirth IS a women’s rights issue and a reproductive issue:
Childbirth is a women’s rights issue and a reproductive justice issue. The United States maternity system is one of the costliest in the developed world, yet our birth outcomes compare poorly to those of other industrialized nations. Among industrialized countries, we consistently rank last or second to last in perinatal and maternal mortality rates. Moreover, birth is depicted in mainstream media with fear, medical intervention, and crisis…
via Business of Being Born: Classroom Edition | Talk Birth.
But, childbirth is also, quite simply, a human issue:
This is the whole point—women’s rights aren’t about “taking” rights from anyone else OR about demanding “special treatment,” they are important for a HUMANE WORLD for all people. I think it is hilariously awful that “women’s rights” are considered a political issue and that there is a section about “women’s rights” in the “opposing viewpoints” database for my social policy class. As long as women’s rights are considered a political issue or as something about which an opposing viewpoint can be held, rather than as self-evident, we are in continued, desperate need of revolution.
via Women’s Power & Self-Authority | Talk Birth.
Human rights in childbirth include access to the provider of one’s own free choice, so on a related note check out this set of consumer-oriented materials about the midwives model of care offered by collaborative effort of several midwifery organizations and endorsed by several others:
“Normal Healthy Childbirth for Women & Families: What You Need to Know” clearly explains and advocates the benefits of normal, physiologic birth for the average health care consumer. This helpful tool was created from a 2012 consensus statement developed by ACNM, the Midwives Alliance of North America, and the National Association of Certified Professional Midwives.
via OMOT Normal Birth Document Feature Page.
The below quote may seem obvious to birth advocates, but it is revolutionary in terms of health care. When Citizens for Midwifery shared this quote, they noted that, “One the KEY findings of the Lancet Special Series on Midwifery affirms the importance of women and their families participating in planning of health care.” For more from this special series on midwifery, go here: TheLancet.com.

And, in case we get so caught up in theorizing about appropriate care that we forget the lived experiences of the women who need it, read this tough, sobering article about why “going in pushing” does not a VBAC birth plan make:
Karen’s story is not uncommon and nor is the advice she was given about “going in pushing” but when we tell women they can not be cut unless they consent are we telling the truth? Whilst it’s true that legally the hospital can not physically force you into an operating theatre without your consent, they are not afraid to gain consent using underhand methods…
via Go In Pushing – It’s not a VBAC Birth Plan – Whole Woman.
And, of course, some relevant quotes to remember:
“If women lose the right to say where and how they birth their children, then they will have lost something that is as dear to life as breathing.” –Ami McKay
“Mothers need to know that their care and their choices won’t be compromised by birth politics.” – Jennifer Rosenberg
via As dear as breathing… | Talk Birth.
Is there anything that can be done, or are we facing an insurmountable struggle? I think we can remember that our “small stone” birth activism does matter:
While reading the book The Mother Trip by Ariel Gore, I came across this quote from civil rights activist Alice Walker: “It has become a common feeling, I believe, as we have watched our heroes failing over the years, that our own small stone of activism, which might not seem to measure up to the rugged boulders of heroism we have so admired, is a paltry offering toward the building of an edifice of hope. Many who believe this choose to withhold their offerings out of shame. This is the tragedy of our world.” Ariel adds her own thoughts to this: “Remember: as women, as mothers, we cannot not work. Put aside your ideas that your work should be something different or grander than it is. In each area of your life—in work, art, child-rearing, gardening, friendships, politics, love, and spirituality—do what you can do. That’s enough. Your small stone is enough.”
These quotes caused me to reflect on the myriad methods of “small stone” birth activism that can be engaged in as a passionate birth activist mother embroiled in a season of her life in which the needs of her own young family take precedence over “changing the world”…
via Small Stone Birth Activism | Talk Birth.
And, on a fun note, you might enjoy this lovely homebirth treasury on etsy: Home Birth by Kayleigh on Etsy. 🙂
“Thousands of women today have had their babies born under modern humanitarian conditions–they are the first to disclaim any knowledge of the beauties of childbirth…” –Grantly Dick Read, Childbirth without Fear
“I am not free while any woman is unfree, even when her shackles are very different from my own.” –Audre Lorde
“Humanizing birth means understanding that the woman giving birth is a human being, not a machine and not just a container for making babies. Showing women—half of all people—that they are inferior and inadequate by taking away their power to give birth is a tragedy for all society.” –Marsden Wagner

 Several months ago, I received an email from one of my former college students. His wife was newly pregnant and they had several specific questions. They asked for my help and recommendations with where to go for answers and without hesitation, I suggested a book: Pregnancy, Childbirth, and the Newborn. I was confident that not only would they find the answers they sought in the book, but also reliable, practical, helpful answers to questions they haven’t even thought to ask yet.
Several months ago, I received an email from one of my former college students. His wife was newly pregnant and they had several specific questions. They asked for my help and recommendations with where to go for answers and without hesitation, I suggested a book: Pregnancy, Childbirth, and the Newborn. I was confident that not only would they find the answers they sought in the book, but also reliable, practical, helpful answers to questions they haven’t even thought to ask yet. drawings illustrating a variety of positions and concepts. This new fifth edition has lots of black and white photos as well. The fact that the book is co-authored by a world-renowned doula, a nurse/lactation consultant, a nurse/childbirth educator, a social worker, and a physical therapist, means it is an interdisciplinary resource benefiting from the skills and professional experience of each co-author. Childbirth educators and doulas as well as pregnant couples will want to check out the companion website which has a plethora of pdf handouts available on numerous topics including comfort techniques, nutrition, and parental leave.
drawings illustrating a variety of positions and concepts. This new fifth edition has lots of black and white photos as well. The fact that the book is co-authored by a world-renowned doula, a nurse/lactation consultant, a nurse/childbirth educator, a social worker, and a physical therapist, means it is an interdisciplinary resource benefiting from the skills and professional experience of each co-author. Childbirth educators and doulas as well as pregnant couples will want to check out the companion website which has a plethora of pdf handouts available on numerous topics including comfort techniques, nutrition, and parental leave.